
…why obesity is not that simple.
It’s that time of year again when people take meaningful stock of their lives and the year that they have just endured. Many are ready to turn over a new leaf after thoughtful reflection and repose; invariably, their health, once again, becomes a priority. For many, that means their weight.
Most know which foods are health promoting and which ones are not, yet struggle to eat the former and eschew the latter while nonchalantly saying, “I know what to do…I just need to do it.” In saying so, they are referencing the apparent simplicity that they have assigned to this shift in eating that they are wanting or yearning for as they know that they will feel better in doing so. And yet, they are most likely to experience challenges with this mindset, as saying ‘so long’ to foods and drinks that are not consistent with their stated health goals is relatively easy as we move through the holiday season that, for many, is filled with an abundance ellof these foods and drinks. But when the last of the holiday food is gone and what’s left are egg whites and yogurt, it feels very different very quickly. Tack on the inclusion of a new workout routine that they also committed to start, and many will simply give up before months’ end. To better understand why this happens, it is important to comprehend the complexity of obesity.
In 1998, the National Institutes of Health (NIH) declared obesity a medical disease. In 2013, the American Medical Association (AMA) followed suit, but added that it required treatment and prevention efforts for those with a BMI >30. Since then, there has been a bonafide tug-o-war within the healthcare industry to acknowledge the legitimacy of obesity being a medical condition and not just a behavior abnormality. Those that recognize obesity as a diagnosis understand the remarkable complexity involved; those that do not are stuck in the decades-old belief that those that are obese simply need to ‘eat less and move more’. If only it were that easy for those who are obese. I have yet to meet someone who has become obese who hasn’t tried that Pollyanna recommendation only to fail and feel the repeated shame associated with not being able to accomplish that which has been framed as a simple way to attain their stated goal. It adds to the stigma and discrimination attached to those with obesity. This is not helpful.
There are myriad reasons why those who experience obesity struggle, and it also isn’t because they ‘just lack discipline’. Genetics, environment, mental health, locus-of-control, health literacy, and restorative sleep all play major roles in contributing to obesity or the ability to lose and keep off the weight. This is why ‘eating less’ may seem to make logical sense at the very novice level of understanding, but fails to address the known competing issues that are at play. What causes an individual to cross over from a normal weight to being obese may have started as a result of consuming too many calories, but we know that once obese for a period of time they cannot simply cut back on those extra calories and return to their normal weight. And it is for sure not because they would prefer to remain obese. No-one seeks out a life of obesity, no different than hoping to grow up with a dependence on alcohol.The parallels are remarkable. And yet, something(s) triggers both and leads to highly undesirable outcomes. Some have genetic predispositions and that likely means a lifelong endeavor of creating a different relationship with food that then allows for the attainment of a healthier weight. The physical and emotional environments in which we grew up in and around are known contributing factors for obesity. This is also true for your life today.
Think about how far you have to travel to find a donut, bagel or caramel swirled hot coffee. It’s likely within a mile or two of your home, but with the super easy ability to all but anonymously order through an app, food is often literally dropped off at your doorstep. Consider how convenience foods have taken over the art of cooking a meal. Our food supply has changed a lot over the past two decades, and it is estimated that greater than 50% of those foods that we eat are largely made up of ultra-processed foods (UPF) manufactured by a handful of food conglomerates (Kraft HeinzCo, Nabisco, Danone, Smithfield, Coca-Cola, PepsiCo, Tyson, Nestle’, Conagra, Mars, Kellogg, Perdue) who ostensibly promote ‘health’ with their catchy labeling when their true goal is simple: to maximize consumption, and in doing so increase sales.
These manufactured foods hijack the brain and makes decision-making extremely challenging to those that are susceptible. And we know this because we see the changes in the brain when exposed to these foods that we do not see when someone eats, for example, an apple. A freshly picked strawberry does not lead to obsessive thoughts, excessive calorie intake, or feeing bad about yourself, but a handful of salted chips or one M&M can and often does. Why can you regulate the amount of berries you eat with ease, yet struggle to close the chip or cookie bag? Why do some not struggle with weight and others define their entire life as having done so? Why do some people eat very few calories, exercise consistently, and yet remain obese? Why are some people always hungry? And what role does privilege play in that those who are financially secure eat fresh fruits, vegetables, lean proteins more often, and are cognizant of their hydration, and, in contrast, those who are financially insecure look to convenience foods and choose from the dollar menu where they can find inexpensive, hyper-palatable foods?
The answer to all these questions are just beginning to be understood. But one hypothesis re: how those with obesity ‘should’ lose weight- balance calories in vs calories out - is now widely recognized as being flawed.We can see initial weight loss if the baseline calorie intake had been very high initially and it then notably dropped; however, weight plateauing (WP) and weight regain (WR) will likely occur, and should be discussed and understood upfront when setting out to lose weight. It allows for a plan to navigate through these challenging biochemical responses and to encourage not giving up. If it is not understood, many will often ‘take a break’ and default to their old ways of eating. They are not lazy in choosing to do so; they are likely emotionally tired of focusing on only eating well. In their tiredness, they may long for their comfort foods from the past.
If those old ways of eating involved high fat, sodium, and refined carbohydrates, they then get a nice dopamine rush that is associated with enjoyment. This neurotransmitter taps into the reward center in the brain and allows them to ‘feel better’ and push aside their sense of discouragement. It is then very easy for the decades-long behaviors that they had so recently been committed to saying ‘good bye’ to to return with a vengeance. What they are likely experiencing is the physiological changes that work against weight loss by triggering appetite-regulating hormones in the stomach, fat cells, pancreas and small intestine. Put simply, they experience being hungry and act upon it just like those with normal weight.
Obesity is a complex diagnosis, but losing weight and successfully keeping it off can happen. And that does not start with a short-lived diet based on restriction, but with a better understanding of your relationship with food and how to navigate around it and in collaboration with the other variables that add to the complexity. Take a few minutes to thoughtfully consider whether your sleep is restorative; if you have a solid baseline understanding of nutrition; if you believe in yourself and that you can lose the weight; and if you have addressed those emotional issues, e.g. depression, anxiety, trauma that may be holding you back from creating a healthier you. If not, this is a great time to do it.
We have to change to become healthier; you already likely know where to begin. And for those working with a colleague, friend, parent or child who is diagnosed with obesity, consider how you can support them best and not be so quick to judge critically. They do enough of that on their own. If you are ready to make some changes to becoming you…only healthier, let me know how I can support you best.

Rosen, Howard. “Is Obesity A Disease or A Behavior Abnormality? Did the AMA Get It Right?.” Missouri medicine vol. 111,2 (2014): 104-108.
Hall, Kevin D et al. “Ultra-Processed Diets Cause Excess Calorie Intake and Weight Gain: An Inpatient Randomized Controlled Trial of Ad Libitum Food Intake.” Cell metabolism vol. 30,1 (2019): 67-77.e3. doi:10.1016/j.cmet.2019.05.008
Fazzino, Tera L et al. “Hyper-Palatable Foods: Development of a Quantitative Definition and Application to the US Food System Database.” Obesity (Silver Spring, Md.) vol. 27,11 (2019): 1761-1768. doi:10.1002/oby.22639.
Forde, Ciarán G et al. “Ultra-Processing or Oral Processing? A Role for Energy Density and Eating Rate in Moderating Energy Intake from Processed Foods.” Current developments in nutrition vol. 4,3 nzaa019. 10 Feb. 2020, doi:10.1093/cdn/nzaa019
© 2022 Audrey L Anastasia. DrPH, RD
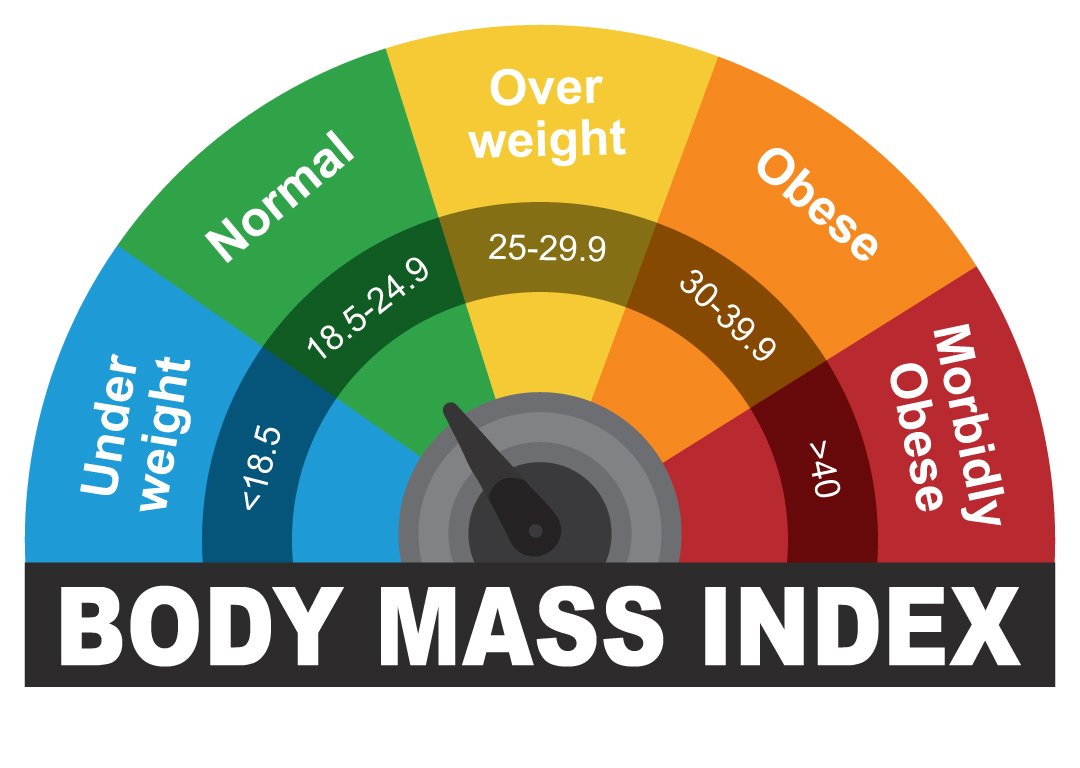
To determine your BMI, check out this link—-> Quick Calculation of My BMI
